What does the United States have in common with Peru, Zimbabwe, Bangladesh, and Uzbekistan? Answer: none of them have a universal health care system. The US is the only country in the developed world that does not provide health care to all of its citizens.
The US federal government actually pays for a lot of health care. If you are old, very poor, or ex-military, the government foots the bill. That’s 37% of the population. But the system is hardly efficient. What the US pays for less than half of its population is more than what every other country pays to look after all their citizens, even after you have adjusted for population size (Norway and the Netherlands are the only exceptions).
Size, culture and politics are barriers to reaching universal healthcare in the US - but aren’t enough to explain why the US doesn’t provide health benefits for all. What does? Vested interests, diversity, and a fortunate history.
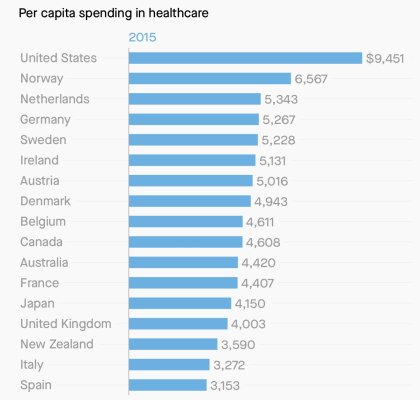
Vested interests. Spending on health care makes up a staggering 17.4% of American GDP. That’s double what Australia or Japan spends, and more than 5% more than its nearest competitor. There are a lot of people making a lot of money from the current health care system in the US. That includes hospitals, doctors, pharmaceutical corporations, and insurance companies. The only way the US could afford universal care would be to cut costs. That would mean confronting some or all of those who benefit from the current state of affairs. That would be very hard. It might even be impossible.
Universal health care works best in countries where people feel strong solidarity with one another. They think that everyone else in society is basically the same as them. But that’s never been the case in the US. The sheer size and cultural diversity of the country, and especially the old and painful divisions over race mean that it’s all too easy for Americans to feel that their fellow citizens are not like them at all. So why should they pay taxes for other people to get looked after?
Most European countries set up universal health systems after the Second World War. So many had died (tens of millions), so many made homeless (tens of millions), so many bereaved (hundreds of millions) that it was hard to argue against the idea that every citizen deserved the chance of a decent, healthy life.
The American experience of the Second World War was very different. 400,000 died, but the country looked better after it than before. The war had brought the US out of the Great Depression and the country was now the leader of the free world. It still had big problems, as the Civil Rights movement would show, but the postwar mood was triumphant, not somber. America was the richest, strongest country ever. It was easy to overlook those who couldn’t afford eyeglasses, let alone surgery.