You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Ebola in Texas
- Thread starter REWahoo
- Start date
Fermion
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
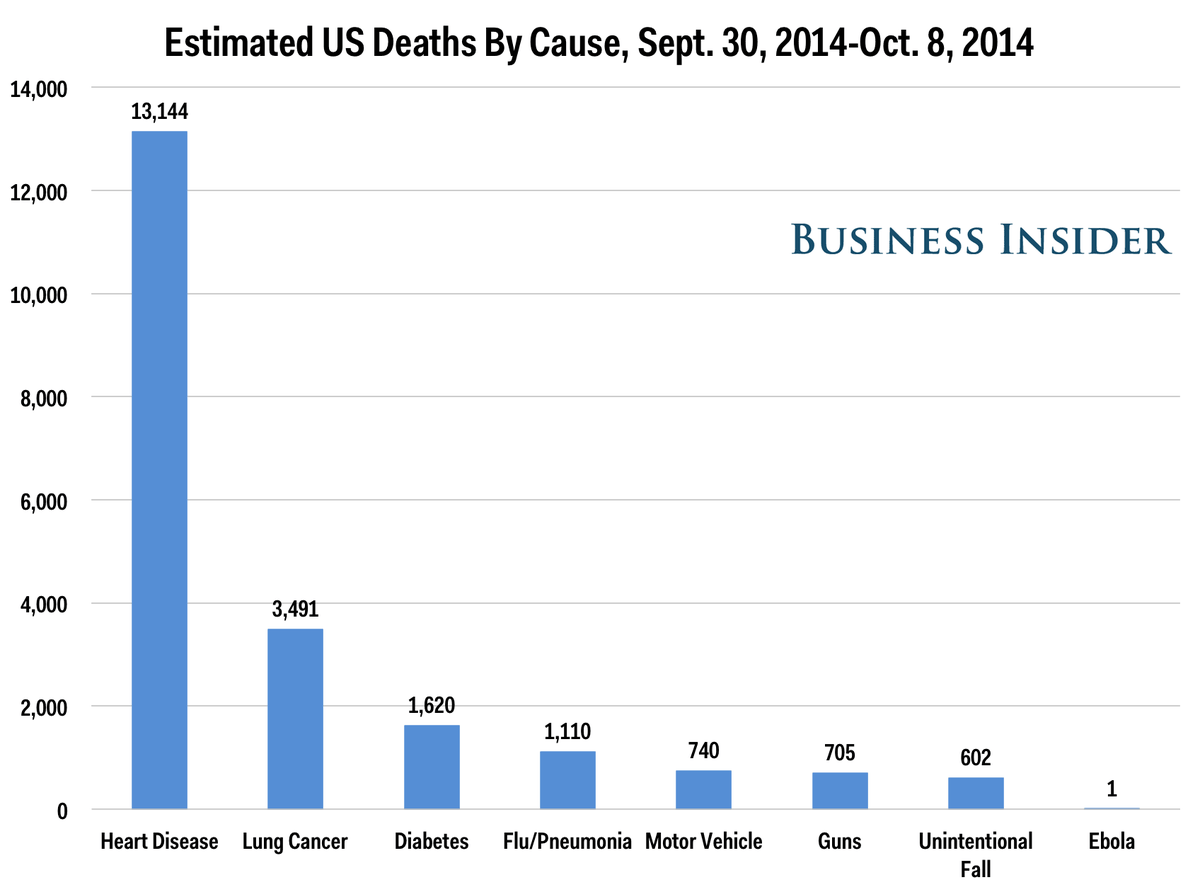
A silly chart because we have not had a outbreak of Ebola in the USA yet.
The whole point of excess caution is so you don't have to revise that chart later.
There is a reason billions will be spent recalling faulty airbags when only four people are known to have died possibly due to their failure. Sometimes you exercise caution before people die.
The whole point of excess caution is so you don't have to revise that chart later.
There is a reason billions will be spent recalling faulty airbags when only four people are known to have died possibly due to their failure. Sometimes you exercise caution before people die.
timo2
Thinks s/he gets paid by the post
There is a reason billions will be spent recalling faulty airbags when only four people are known to have died possibly due to their failure. Sometimes you exercise caution before people die.
People are willing to believe the safety experts regarding air bags, but ignore the medical experts and epidemiologists regarding Ebola. I don't understand that disconnect?
- Joined
- Oct 13, 2010
- Messages
- 10,735
I think I understand it, and it's apples and oranges, IMHO.People are willing to believe the safety experts regarding air bags, but ignore the medical experts and epidemiologists regarding Ebola. I don't understand that disconnect?
If the subset of experts in the anti-quarantine camp are wrong, the consequences could be exponentially horrific (if, by some chance, the virus "gets loose", thousands? millions?, who knows? will die).
If the anti-recall experts are wrong, it might mean we collect another couple of years worth of data and maybe a handful of people die, at most.
So the possible consequences of being conservative in the two cases are as different as night and day.
People are willing to believe the safety experts regarding air bags, but ignore the medical experts and epidemiologists regarding Ebola. I don't understand that disconnect?
Physics, electronics, and vehicle accident rates= "hard" science. Experimental method = easily applied
Ebola, biological processes, societal responses to infection = "soft" science.
"Hard" science is more easily tested, more quantifiable, and more easily understood. Experimental method often requires retrospective analysis, time, and trying to control for variables that invariably reduce the faith we can have in the results.
It's clear that the situation is entirely different.
Last edited:
meierlde
Thinks s/he gets paid by the post
I think I understand it, and it's apples and oranges, IMHO.
If the subset of experts in the anti-quarantine camp are wrong, the consequences could be exponentially horrific (if, by some chance, the virus "gets loose", thousands? millions?, who knows? will die).
If the anti-recall experts are wrong, it might mean we collect another couple of years worth of data and maybe a handful of people die, at most.
So the possible consequences of being conservative in the two cases are as different as night and day.
I understand a large part of the problem in West Africa is the way bodies are prepared for burial. The family must wash the body, which at that point is a great way to get the disease. This is like folks in the US handled death 150 years ago (see the number of family plots etc.).
timo2
Thinks s/he gets paid by the post
Physics, electronics, and vehicle accident rates= "hard" science. Experimental method = easily applied
Ebola, biological processes, societal responses to infection = "soft" science.
"Hard" science is more easily tested, more quantifiable, and more easily understood. Experimental method often requires retrospective analysis, time, and trying to control for variables that invariably reduce the faith we can have in the results.
It's clear that the situation is entirely different.
The point I'm making does not involve nuanced differences of the subject matter, but the cafeteria style approach as to which 'experts' people believe. The disconnect I'm seeing is that the same overarching scientific establishment (scientific industrial complex?) that created our modern civilization - vaccines, penicillin, computers, space exploration, heart transplants - is only believed when people 'feel' like they agree with the scientific determination. It turns out Ebola is one of those scientific determinations that people just 'feel' is wrong, for whatever reason, without any actual proof for their skepticism. That's the disconnect I see.
EastWest Gal
Thinks s/he gets paid by the post
I wonder why someone returning from a high risk situation (treating ebola patients) is not simply automatically blood tested for the virus upon his return, rather than having him self-monitor and/or voluntarily quarantine for 21 days to see if symptoms develop?
The virus, like all viruses, has an incubation period. During that time, the virus is undetectable by any means, and the person is not contagious at all. The problem here is that we don 't have precise information about the minimum incubation period and if there is any contagiousness possible prior to onset of symptoms.
For example we know that with chicken pox, a susceptible person will start the rash 10-21 days after exposure, no more and no less. We also know that a person is contagious up to two days prior to onset of the rash, and it is spread by respiratory droplet-you can't get it at a significant distance, unlike measles, which is truly airborne. So a person exposed to chicken pox should be quarantined from immunocompromised people for 8-21 days. There is a defined period of contagiousness after the rash starts as well. 5-14 days, usually 8 or less.
With ebola, much less is known. I ran across a study from the last outbreak which makes me wonder how much our CDC folks know or bother to search. The paper suggested to reduce the risk to <1% one should use a maximum incubation of 25 days, not 21 days. And the authors failed to commit to a minimum incubation period--which is too bad.
That doctor in NYC was very foolish, going bowling and taking the subway.
Here is the article, though it's a difficult read:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3766904/#!po=78.3582
Sent from my iPhone using Early Retirement Forum
- Joined
- Apr 14, 2006
- Messages
- 23,059
The virus, like all viruses, has an incubation period. During that time, the virus is undetectable by any means, and the person is not contagious at all. The problem here is that we don 't have precise information about the minimum incubation period and if there is any contagiousness possible prior to onset of symptoms.
For example we know that with chicken pox, a susceptible person will start the rash 10-21 days after exposure, no more and no less. We also know that a person is contagious up to two days prior to onset of the rash, and it is spread by respiratory droplet-you can't get it at a significant distance, unlike measles, which is truly airborne. So a person exposed to chicken pox should be quarantined from immunocompromised people for 8-21 days. There is a defined period of contagiousness after the rash starts as well. 5-14 days, usually 8 or less.
With ebola, much less is known. I ran across a study from the last outbreak which makes me wonder how much our CDC folks know or bother to search. The paper suggested to reduce the risk to <1% one should use a maximum incubation of 25 days, not 21 days. And the authors failed to commit to a minimum incubation period--which is too bad.
That doctor in NYC was very foolish, going bowling and taking the subway.
Here is the article, though it's a difficult read:
Incubation Period of Ebola Hemorrhagic Virus Subtype Zaire
Sent from my iPhone using Early Retirement Forum
Thanks, I suspected it was something like that. Here is an article about a nurse in Connecticut who seems to have done things the right way.
Tolland Nurse Just Back From Treating Patients With Ebola In W. Africa - Hartford Courant
Your link just takes me to a home page for the newspaper. I'm assuming this is the nurse that fought NJ's quarantine. It will be interesting what happens should this nurse develop symptoms later.Thanks, I suspected it was something like that. Here is an article about a nurse in Connecticut who seems to have done things the right way.
Tolland Nurse Just Back From Treating Patients With Ebola In W. Africa - Hartford Courant
I'm sure there have been many dozens of heathcare workers that came back from West Africa without issues. Unfortunately, we've just seen one that didn't.
eytonxav
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
Y I'm assuming this is the nurse that fought NJ's quarantine.
No, the nurse you are referring to was from Maine, the one Gumby posted about is from Connecticut.
timo2
Thinks s/he gets paid by the post
Apparently not all bodily fluids are the same
A Glossary of Ebola Contact Types - Defense - GovExec.com
"Since Ebola made landfall in the US in September, officials at the US Centers for Disease Control and their counterparts at the state and local levels have campaigned to educate the public about how the virus can—and can’t—move from person to person. The effort has resulted in communiqués about the difference between “casual,” “direct” and “close” contact. With that in mind, here is a guide to help you stay Ebola-free while maintaining whatever interaction with others you (and they) prefer."
A Glossary of Ebola Contact Types - Defense - GovExec.com
"Since Ebola made landfall in the US in September, officials at the US Centers for Disease Control and their counterparts at the state and local levels have campaigned to educate the public about how the virus can—and can’t—move from person to person. The effort has resulted in communiqués about the difference between “casual,” “direct” and “close” contact. With that in mind, here is a guide to help you stay Ebola-free while maintaining whatever interaction with others you (and they) prefer."
HFWR
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
A friend of a friend in the nursing profession posted this on Facebook not long ago...
I've been watching the news a lot the past few days and I've noticed something. I think those who don't work in the medical profession don't understand how difficult it is to actually contract the Ebola virus.
Here is a list of all the people in America who were infected with Ebola virus disease:
Dr. Kent Brantly
Dr. Rick Sacra
Nancy Writebol
Eric Duncan
Nina Pham
Amber Vinson
There is one thing that all of these people have in common. They were in direct contact with the vomit and feces of someone who was in the later stages of infection with the Ebola virus. Dr Sacra contracted the disease after performing a c-section on a patient (in LIberia) who had not yet been diagnosed with the disease.
And, other than playing with infected bats and monkeys, that is the only way to get it.
But why has the Ebola virus killed thousands in African countries?
Because these are third-world countries. Most of the "hospitals" where their Ebola patients spend their last days don't have working sewer systems. They don't have disposable bedpans and advanced waste-management systems like we do in the US.
A little look into the relationship between a critically ill patient and their healthcare team will also be helpful. This is not for the weak of stomach.
When a patient is in the last stages of their battle with the Ebola virus, they produce a large amount of mucous, stool, vomit, and possibly blood. When a patient who is unable to sit up or get out of bed is stricken with these symptoms, I can assure you that these substances get EVERYWHERE. We're not talking a couple of bowel movements a day. We're talking about a constant flow of liquid stool coming from a patient who can only lie in the bed as it pools around them. And every time you change those sheets - which requires two people - you have piles of poop-covered sheets and gowns moved all around the room.
On several occasions during my career as an ICU nurse, I have found myself asking the question, "How in the hell did poop get THERE?"
And if the actual virus is IN the poop, then you're getting that virus on EVERYTHING.
And all these people in ties and skirts have never been at the bedside cleaning these messes. They do not understand the situation that these caregivers are in any more than a fish knows what it's like to sneeze. So when they get in front of a camera yack about Ebola, you need to take it with a grain of salt and check the facts for yourself.
My point is this: Although the Ebola virus disease IS a serious illness, the media is seriously exaggerating the actual danger to you and your family. Unless you are literally cleaning up the poop or vomit of someone who is dying from Ebola virus disease, you're safe.
Last edited:
Fermion
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
Will someone please answer the question of how the American journalist covering the Ebola outbreak came down with the disease when he said he exercised caution while filming?
Did he have sex with monkeys or clean his camera lens with infected poop?
It just doesn't sound like he was doing C-sections or cleaning bedpans, or even licking corpses.
Did he have sex with monkeys or clean his camera lens with infected poop?
It just doesn't sound like he was doing C-sections or cleaning bedpans, or even licking corpses.
timo2
Thinks s/he gets paid by the post
Will someone please answer the question of how the American journalist covering the Ebola outbreak came down with the disease when he said he exercised caution while filming?
Did he have sex with monkeys or clean his camera lens with infected poop?
It just doesn't sound like he was doing C-sections or cleaning bedpans, or even licking corpses.
I take it to mean that his perception of what he did is different from his reality. IMHO.
Bestwifeever
Moderator Emeritus
- Joined
- Sep 17, 2007
- Messages
- 17,774
He apparently told his father he was spraying his shoes with a hose to clean them off after being in the medical area (his father said he told him that but he hasn't mentioned it himself to the press), and some of the contaminated water splashed on his bare skin.
Last edited:
FireBug
Recycles dryer sheets
The point I'm making does not involve nuanced differences of the subject matter, but the cafeteria style approach as to which 'experts' people believe. The disconnect I'm seeing is that the same overarching scientific establishment (scientific industrial complex?) that created our modern civilization - vaccines, penicillin, computers, space exploration, heart transplants - is only believed when people 'feel' like they agree with the scientific determination. It turns out Ebola is one of those scientific determinations that people just 'feel' is wrong, for whatever reason, without any actual proof for their skepticism. That's the disconnect I see.
+1
- Joined
- Apr 14, 2006
- Messages
- 23,059
Your link just takes me to a home page for the newspaper. I'm assuming this is the nurse that fought NJ's quarantine. It will be interesting what happens should this nurse develop symptoms later.
I'm sure there have been many dozens of heathcare workers that came back from West Africa without issues. Unfortunately, we've just seen one that didn't.
That's odd. When I click on the link, it goes to the article. In any event, the nurse in Tolland worked with Ebola patients in Sierra Leone. When she returned to Connecticut, she voluntarily quarantined herself on her son's farm for three weeks, feeding the chickens, reading and doing chores but avoiding direct physical contact with her family. After the 21 days were up, they had a dinner party. No fuss, no threats of lawsuits, just a responsible woman doing what needed to be done. She is now down in Atlanta training CDC workers how to dress and undress in the personal protective equipment.
Fermion
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
He apparently told his father he was spraying his shoes with a hose to clean them off after being in the medical area (his father said he told him that but he hasn't mentioned it himself to the press), and some of the contaminated water splashed on his bare skin.
Well that certainly doesn't sound like he was directly exposed as those in this thread contend you need to be to contract this virus.
The virus was on his shoes, he sprayed them with water and got some backsplash, the 80nm virus traveled in the water droplet to his skin, then he rubbed his eye within a few hours. Something like that?
Doesn't sound incredibly different from a returning healthcare worker using a public bathroom at, say, a bowling alley, spreading the virus from their rectum region to the toilet seat or stall door, then having the next person who uses the bathroom pick up the virus and rub their eye.
It is not a far fetched scenario at all in my opinion. Especially if the worker is right on the edge of symptomatic or is one of the small percentage that do not readily show symptoms. If the virus is already in the stool then it can be spread fairly easily.
EastWest Gal
Thinks s/he gets paid by the post
He apparently told his father he was spraying his shoes with a hose to clean them off after being in the medical area (his father said he told him that but he hasn't mentioned it himself to the press), and some of the contaminated water splashed on his bare skin.
Water doesn't kill ebola, and so he no doubt splashed it around. Should have used a bleach solution. Ruined shoes is a small price to pay to prevent ebola. Hope he didn't infect anyone else.
Bestwifeever
Moderator Emeritus
- Joined
- Sep 17, 2007
- Messages
- 17,774
I wonder if all the caregivers to the Dallas nurses, the photojournalist, and the Doc w/o borders are being quarantined. I guess they should be too?
MooreBonds
Thinks s/he gets paid by the post
It somewhat reminds of the hysteria, when AIDs first hit the scene. People with HIV were fired, kids weren't allowed to go to school, lots of bans were proposed with respect to gays. The panic was understandable in many ways, a highly lethal disease with no cure and no treatment. AIDs actually is lot scary than Ebola even today. It appears with prompt medical help in a Western hospital you are very likely to survive Ebola and after a few weeks are pretty healthy again.
The ultimate solution with HIV/AIDs was education, not knee jerk reactions.
The big difference is that over a span of just 10-20 days (possibly fewer), nearly every HIV/AIDs patient doesn't develop massive diarrhea, or blood hemorrhaging out of their eyes/orifices, and profuse sweating (which might include traces of blood, but either way could include the virus), and doesn't have projectile vomiting of blood - all filled with the virus.
If that were the case for 99.9% of HIV patients, do you think they would have merely resorted to 'education'?
And in today's news that really doesn't make sense:
White House: 'Not unusual' for Ebola quarantine rules to differ for military, general population - Washington Times
So you have military service men and women who were NOT directly treating or interacting with or even anywhere near any Ebola patients, who were merely in the same country as Ebola victims, who are required to have strict isolation quarantine for 21 days upon leaving the Ebola country.
Yet, healthcare workers directly treating Ebola patients should not have any quarantine whatsoever....according to this administration.
- Joined
- Apr 14, 2006
- Messages
- 23,059
A. The military rarely does anything by half-measures; and
B. It is substantially easier to violate the constitutional rights of military members than civilians.
B. It is substantially easier to violate the constitutional rights of military members than civilians.
photoguy
Thinks s/he gets paid by the post
- Joined
- Jun 15, 2010
- Messages
- 2,301
Interesting editorial on the quarantine in the New England Journal of Medicine:
NEJM Editorially link
NEJM Editorially link
Therefore, an asymptomatic health care worker returning from treating patients with Ebola, even if he or she were infected, would not be contagious. Furthermore, we now know that fever precedes the contagious stage, allowing workers who are unknowingly infected to identify themselves before they become a threat to their community. This understanding is based on more than clinical observation: the sensitive blood polymerase-chain-reaction (PCR) test for Ebola is often negative on the day when fever or other symptoms begin and only becomes reliably positive 2 to 3 days after symptom onset. This point is supported by the fact that of the nurses caring for Thomas Eric Duncan, the man who died from Ebola virus disease in Texas in October, only those who cared for him at the end of his life, when the number of virions he was shedding was likely to be very high, became infected. Notably, Duncan's family members who were living in the same household for days as he was at the start of his illness did not become infected.
A cynic would say that all these “facts” are derived from observation and that it pays to be 100% safe and to isolate anyone with a remote chance of carrying the virus. What harm can that approach do besides inconveniencing a few health care workers? We strongly disagree. Hundreds of years of experience show that to stop an epidemic of this type requires controlling it at its source. Médecins sans Frontières, the World Health Organization, the U.S. Agency for International Development (USAID), and many other organizations say we need tens of thousands of additional volunteers to control the epidemic. We are far short of that goal, so the need for workers on the ground is great. These responsible, skilled health care workers who are risking their lives to help others are also helping by stemming the epidemic at its source. If we add barriers making it harder for volunteers to return to their community, we are hurting ourselves.
clifp
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- Oct 27, 2006
- Messages
- 7,733
Interesting editorial on the quarantine in the New England Journal of Medicine:
NEJM Editorially link
I agree with the New England Journal. It is pretty clear that disease only spreads when the Ebola victim is obviously sick. Not only did none of Thomas Duncan family or friends get sick, but neither did any of the 132 passenger of Frontier Airline, who flew with Amber Vinson, nor any of Nurse Nina Pham contacts. I'd be willing to bet none of the people who were in contact with bowling Doctor in NY will be infected either.
Doctors without border has had more than 700 staff members treat people with Ebola and they have had exactly one staff member return home without symptoms and then develop the disease.
I think history will show the folks calling for a quarantine to be just as foolish as the mothers who insisted that kids with HIV stay home from school, cause the kid might get a nose bleed.