I think there are a number of factors at play. And as the pandemic plays out, and more data is collected, a better picture will emerge.
First, the key in figuring out the OP ? is to understand the disease process. And this itself is still being understood. But it looks like there is an inoculating event, then a period (very extended for a human virus) where the virus is replicating and during this period the human is also just “trying” to figure out what is going on, and then there is the “battle” period between the host and virus. At each of these points, and at each point along this process, the virus, or the host, could have the advantage. The ultimate goal is for the human to gain the upper hand and defeat the virus.
So starting from the beginning, if the inoculating dose is very large, then the exponential growth of the virus overwhelms the human’s opportunity and time-frame to mount a successful battle. This may have happened eg. in Dr. Li WianLiang, who as an ophthalmologist, was seeing multiple patients, very up close, just inches from the faces of people who were sick/asymptomatic carriers. This may have also happened in the cases of ED physicians and hands-on nurses who passed away, though healthy, after encountering massive, or repeated large inoculum doses. And it is also suggested by some studies from Italy, where it’s showing that elderly people who got COVID from live-in COVID family had a higher chance of dying, presumably because they were exposed to larger doses when co-habitating than say, randomly handing the same banister in an apt bldg stairwell.
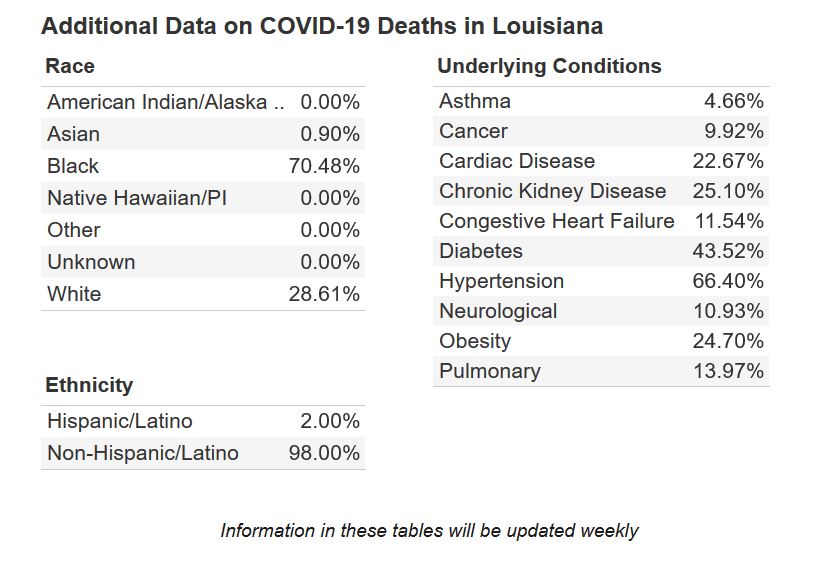
Then there is the question of ACE2 receptors being the landing pad of SARS-CoV2. So smokers are at increased risk, and this is presumed in part due to their ACE2 receptors being up-regulated. And presumably there is genetic variation of ACE2 expression too. Not sure how much this will be shown in AA populations, as (IMO) all the other possible reasons are more probable (having front-line/essential jobs such as bus driver, janitorial staff in hospitals, etc).
Then once the virus gets into your body, how well does your body function? As an organism? So SARS-CoV2 has been shown to directly attack lungs (everybody knows this one), your kidneys, heart, brainstem and possibly meninges, and liver. So a baseline problem in any of those organs would be disadvantageous. Diabetes is a problem because it decreases your immune system well-functioning, and it also damages almost every organ in your body. Obesity is a problem because of a number of different reasons, but the most obvious would be that it makes the body less efficient in what it needs to do, and specifically regarding breathing, causes a significant extra load on breathing, which can become very problematic in full blown COVID (even w/o the obesity).
The last stage of the disease process, where the body is mounting an immune response to SARS-CoV2, that immune process can go overboard, a.k.a. cytokine storm. This may be the puzzler in seemingly young, healthy people dying.
Things that suppress your immune system would also be disadvantageous, eg. pregnancy, body fighting cancer, body on chemo, kidney disease.