explanade
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- May 10, 2008
- Messages
- 7,448
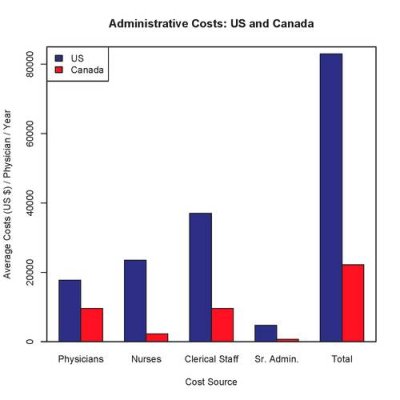
I have always thought that there are many facets to the issue of high health care costs in the US. Here's another example. In both my family doctor and my dentist offices, I saw about the same number of clerical workers as the number of health care professionals, i.e. nurses or PA and the doctor himself. Obviously, they need many paper pushers to deal with Medicare and the private insurance companies. And then, on the other end, who knows how many are employed by the government and the insurance companies to haggle back and forth with the health care providers. Meanwhile, do the patients know if the charges are correct, or do they even care how much certain procedures cost?
There was a famous Harvard Medical School study a few years ago which estimated that at least 25% of our total health care spending goes to processing insurance claims. We're talking half a trillion per year or more.
Doctors have to hire full-time staff to process insurance payments, as different insurers use different codes for the same conditions. Even then, many doctors have to spend a big chunk of their time handling the insurance claims as well.
Oddly though, during the whole health care debate, it was pointed out that the total revenues of all health insurance carriers was a small fraction of total health care spending, under 10% IIRC. But then the processing of the insurance takes a lot of time and money.