You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Who’s Really At Risk of Dying From Covid-19
- Thread starter Midpack
- Start date
- Status
- Not open for further replies.
Related article from India Times regarding the Sweden Model:
https://timesofindia.indiatimes.com...-one-choice-anders-tegnells-swedish-approach/
Where I live (~75% Asian), many wear facemasks all the time. Perhaps this is something those with pre-existing/compromised health conditions consider in the future.
The virus enters the cell via the pathway of ACEs. ACEs are found to be in the nasal passages. If ever found out, it'll be interesting where the virus enters the body. But the virus' final entry into the cells is where ACEs are located--brain stem, heart, lungs, etc.
https://timesofindia.indiatimes.com...-one-choice-anders-tegnells-swedish-approach/
Where I live (~75% Asian), many wear facemasks all the time. Perhaps this is something those with pre-existing/compromised health conditions consider in the future.
The virus enters the cell via the pathway of ACEs. ACEs are found to be in the nasal passages. If ever found out, it'll be interesting where the virus enters the body. But the virus' final entry into the cells is where ACEs are located--brain stem, heart, lungs, etc.
Lienlord
Recycles dryer sheets
The fact they've only been testing the very sick, and comparing the deaths to those testing positive has greatly skewed the rate.
I told someone it's like testing the blood alcohol all the occupants of a bar at 2:00 AM and concluding 40% of the US population are alcoholics!
I told someone it's like testing the blood alcohol all the occupants of a bar at 2:00 AM and concluding 40% of the US population are alcoholics!
Last edited:
Amethyst
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- Dec 21, 2008
- Messages
- 12,668
Everyone seems so focused on deaths, when from what I've read, there can be some pretty terrible outcomes for survivors. Permanent lung scarring is one ghastly outcome. I wish CDC would share more data on those outcomes, assuming they even track them.
When I was 25, I picked up a respiratory virus which I thought was a bad cold. Unfortunately, it attacked my olfactory nerve. To this day I have only 30% normal olfactory/gustatory sensation. Those of you who really love food and wine will appreciate what a sorry thing this is to live with. I recall the neurologist telling me that viruses can attack even our most essential nerves, for hearing, sight, movement.
Viruses are nothing to mess with, and death is not the only miserable outcome to avoid.
When I was 25, I picked up a respiratory virus which I thought was a bad cold. Unfortunately, it attacked my olfactory nerve. To this day I have only 30% normal olfactory/gustatory sensation. Those of you who really love food and wine will appreciate what a sorry thing this is to live with. I recall the neurologist telling me that viruses can attack even our most essential nerves, for hearing, sight, movement.
Viruses are nothing to mess with, and death is not the only miserable outcome to avoid.
Ready
Thinks s/he gets paid by the post
Everyone seems so focused on deaths, when from what I've read, there can be some pretty terrible outcomes for survivors. Permanent lung scarring is one ghastly outcome. I wish CDC would share more data on those outcomes, assuming they even track them.
How could they track the long term health effects of a virus that just appeared in humans for the first time several months ago?
Amethyst
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- Dec 21, 2008
- Messages
- 12,668
Even more to the point, how can we afford to think a couple months' statistics are enough to make life-and-death political decisions?
I realize long-term tracking isn't yet possible. Still, it's known that certain patients are leaving the hospital alive, yet with serious lung scarring that may never go away. That is something the hospital/CDC could track. And it won't be long till we are at the 6-month point, where conditions start to be considered "chronic." That is when my doctor surmised, for example, that my senses of taste and smell were never coming back.
I realize long-term tracking isn't yet possible. Still, it's known that certain patients are leaving the hospital alive, yet with serious lung scarring that may never go away. That is something the hospital/CDC could track. And it won't be long till we are at the 6-month point, where conditions start to be considered "chronic." That is when my doctor surmised, for example, that my senses of taste and smell were never coming back.
How could they track the long term health effects of a virus that just appeared in humans for the first time several months ago?
I'm not so sure society will heed the message of taking control of one's health. The Type II diabetes epidemic is entirely preventable with a low carb diet and exercise. People continue to ignore that fact.Exactly!
I think society will get there eventually once the fear subsides.
BTW In my state, the total March 2020 deaths were much less (ie 30%) than the average of the prior few March(s).
LOL!
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- Jun 25, 2005
- Messages
- 10,252
What are the reference rates for co-mordibity? For example, if around 64% of people over age 60 have hypertension and around 64% of the hospitalized folks over age 60 die of Covid-19, then hypertension would not seem to be a factor. Am I thinking about it the right way?
CardsFan
Thinks s/he gets paid by the post
What are the reference rates for co-mordibity? For example, if around 64% of people over age 60 have hypertension and around 64% of the hospitalized folks over age 60 die of Covid-19, then hypertension would not seem to be a factor. Am I thinking about it the right way?
That was exactly my point in post #59.
Correlation is not causation.
Obviously, it doesn't help. But if you look at the numbers in previous links, the people with co-morbidity number 250%, mean many (most?) had more than one.
But if the percentage of normal 65 year old with hypertension is very close to the stated average, then, is that really a factor?
Of course there are "statistics, damned statistics, and lies"
OP
OP
Midpack
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
You’ve said this a couple times, I assume you’re talking about ARDS, do you have more info? How probable, 6.5% of Covid-19 patients who don’t die? From what little I found most patients who develop ARDS die. It’s much less common in survivors, not that it’s OK for those left alive with ARDS. IOW lung scarring among survivors isn’t common? And is ARDS correlated with comorbidity - just asking?Everyone seems so focused on deaths, when from what I've read, there can be some pretty terrible outcomes for survivors. Permanent lung scarring is one ghastly outcome. I wish CDC would share more data on those outcomes, assuming they even track them.
https://health.clevelandclinic.org/heres-the-damage-coronavirus-covid-19-can-do-to-your-lungs/As Dr. Mukhopadhyay explains, Chinese researchers have linked COVID-19 to ARDS. Their study examined risk factors for 191 confirmed coronavirus patients who died while being treated in two hospitals in Wuhan, China.
The researchers found 50 of the 54 patients who died had developed ARDS while only nine of the 137 survivors had ARDS.
“It’s a really, really significant contribution to death in these patients,” says Dr. Mukhopadhyay.
Last edited:
athena53
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- May 11, 2014
- Messages
- 7,377
What are the reference rates for co-mordibity? For example, if around 64% of people over age 60 have hypertension and around 64% of the hospitalized folks over age 60 die of Covid-19, then hypertension would not seem to be a factor. Am I thinking about it the right way?
The one article for which I read the abstract (found after a search on "COVID-19 Co-Morbidities") did mention adjusting by age. I assume that means that they looked at what % of all people in an age group were obese, had HBP, etc. compared to what % of the ones in that age group who died of COVID-19 had that condition.
Last edited:
copyright1997reloaded
Thinks s/he gets paid by the post
That was exactly my point in post #59.
Correlation is not causation.
Obviously, it doesn't help. But if you look at the numbers in previous links, the people with co-morbidity number 250%, mean many (most?) had more than one.
But if the percentage of normal 65 year old with hypertension is very close to the stated average, then, is that really a factor?
Of course there are "statistics, damned statistics, and lies"
We would need to know:
Hyper Tension + Death %
Hyper Tension No Death %
No Hyper Tension + Death %
No Hyper Tension No Death %
Amethyst
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- Dec 21, 2008
- Messages
- 12,668
https://www.webmd.com/lung/what-does-covid-do-to-your-lungs#2
"Some people had a cough even after they recovered from COVID-19. Others had scarring in their lungs. Doctors are still studying whether these effects are permanent or might heal over time.
Have not yet seen statistics, nor demographic correlations. I think early reporting is focused on deaths, not survivors' conditions.
"Some people had a cough even after they recovered from COVID-19. Others had scarring in their lungs. Doctors are still studying whether these effects are permanent or might heal over time.
Have not yet seen statistics, nor demographic correlations. I think early reporting is focused on deaths, not survivors' conditions.
You’ve said this a couple times, I assume you’re talking about ARDS, do you have more info? How probable, 6.5% of Covid-19 patients who don’t die? From what little I found most patients who develop ARDS die. It’s much less common in survivors, not that it’s OK for those left alive with ARDS. IOW lung scarring among survivors isn’t common? And is ARDS correlated with comorbidity - just asking?
https://health.clevelandclinic.org/heres-the-damage-coronavirus-covid-19-can-do-to-your-lungs/
CardsFan
Thinks s/he gets paid by the post
We would need to know:
Hyper Tension + Death %
Hyper Tension No Death %
No Hyper Tension + Death %
No Hyper Tension No Death %
Yes, we would. Got any data?
Let's face it. Almost ALL data in a case like this will be a long time after the fact.
Right now, we are looking at factiods and bits of data.
NW-Bound
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- Jul 3, 2008
- Messages
- 35,712
I don't watch TV, but I just watched the above clip. What Dr. Scott Jensen was describing was the CDC guideline. We do not know what the coroners in different areas do when filling out the death certificates.
I have read a few articles in the media such as the BBC and AP News which specifically said that a positive result from a PCR test was required as customarily done. Hence, the virus deaths were undercounted.
Last edited:
NW-Bound
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- Jul 3, 2008
- Messages
- 35,712
It did not take me long to find the CDC guideline discussed above. A quick glance through it, and I found this excerpt:
"In cases where a definite diagnosis of COVID–19 cannot be made, but it is suspected or likely (e.g., the circumstances are compelling within a reasonable degree of certainty), it is acceptable to report COVID–19 on a death certificate as “probable” or “presumed.” In these instances, certifiers should use their best clinical judgement in determining if a COVID–19 infection was likely. However, please note that testing for COVID–19 should be conducted whenever possible".
Note the words "probable" and "presumed".
See: https://www.cdc.gov/nchs/data/nvss/vsrg/vsrg03-508.pdf.
By the way, this is not without precedents. On 2/12/2020, China's reported case counts jumped from 44,653 to 58,761. This caused a surprise until it was reported that China decided to re-classify cases with severe lung damage consistent with COVID-19 as observed with a CAT scan.
And it should be noted that horrendous lung damage was what caused some Chinese doctors in Wuhan to sound the initial alarm bell back in Dec 2019, that what they saw was no normal influenza.
In France, on 4/3/2020 the case count jumped from 59,105 to 82,165, while the death count jumped up by 1,120. It was reported that the counts from nursing homes were previously not included. No other details were offered.
"In cases where a definite diagnosis of COVID–19 cannot be made, but it is suspected or likely (e.g., the circumstances are compelling within a reasonable degree of certainty), it is acceptable to report COVID–19 on a death certificate as “probable” or “presumed.” In these instances, certifiers should use their best clinical judgement in determining if a COVID–19 infection was likely. However, please note that testing for COVID–19 should be conducted whenever possible".
Note the words "probable" and "presumed".
See: https://www.cdc.gov/nchs/data/nvss/vsrg/vsrg03-508.pdf.
By the way, this is not without precedents. On 2/12/2020, China's reported case counts jumped from 44,653 to 58,761. This caused a surprise until it was reported that China decided to re-classify cases with severe lung damage consistent with COVID-19 as observed with a CAT scan.
And it should be noted that horrendous lung damage was what caused some Chinese doctors in Wuhan to sound the initial alarm bell back in Dec 2019, that what they saw was no normal influenza.
In France, on 4/3/2020 the case count jumped from 59,105 to 82,165, while the death count jumped up by 1,120. It was reported that the counts from nursing homes were previously not included. No other details were offered.
Last edited:
Freedom56
Thinks s/he gets paid by the post
You don’t need BMI data thru Apr 10th. Relatively few young people have died from Covid-19 including any who are obese, with underlying health issues or any other issues. Again, 90% of the deaths are 55 and over. Those younger who have died we’re likely obese or otherwise health compromised - but even so there have been relatively few - only 10% of deaths have been ages 0 thru 54...
This supports what I posted before:
NYU scientists: Largest U.S. study of COVID-19 finds obesity the single biggest factor in New York City's hospitalizations
Doctors at NYU Langone Health center conducted the largest study so far of U.S. hospital admissions for COVID-19, focused on New York City. They found obesity, along with age, was the biggest deciding factor in hospital admissions, which may suggest the role of hyper-inflammatory reactions that can happen in those with the disease.
https://www.zdnet.com/article/nyu-s...le-biggest-factor-in-new-york-critical-cases/
gauss
Thinks s/he gets paid by the post
- Joined
- Aug 17, 2011
- Messages
- 3,615
^
Anecdotally, reviewing news articles, with photos, of those who have died from this, appears to indicate obesity more often than not.
Anecdotally, reviewing news articles, with photos, of those who have died from this, appears to indicate obesity more often than not.
OP
OP
Midpack
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
So maybe your link matches mine pretty closely, preliminary data though? Certainly nothing to take lightly, but good to know it may only affect 5-6.5% of critical Covid-19 cases - and not a larger group. Thanks.https://www.webmd.com/lung/what-does-covid-do-to-your-lungs#2
"Some people had a cough even after they recovered from COVID-19. Others had scarring in their lungs. Doctors are still studying whether these effects are permanent or might heal over time.
Have not yet seen statistics, nor demographic correlations. I think early reporting is focused on deaths, not survivors' conditions.
Critical Cases
In critical COVID-19 -- about 5% of total cases -- the infection can damage the walls and linings of the air sacs in your lungs. As your body tries to fight it, your lungs become more inflamed and fill with fluid. This can make it harder for them to swap oxygen and carbon dioxide.
You might have severe pneumonia or acute respiratory distress syndrome (ARDS). In the most critical cases, your lungs need help from a machine called a ventilator to do their job.
Turbo29
Full time employment: Posting here.
Don't leave out the medial and allied industries. While the Gov might have it's proprietary reasons to hype/misrepresent/spin these things, the Gov takes money from Business entities to further those interests. The so caled "private sector" is not innocent or uninvolved. They are motivators of these behaviors
The whole situation reminds me of the quote from Smedley Butler's War is a Racket.
" A racket is best described, I believe, as something that is not what it seems to the majority of the people. Only a small "inside" group knows what it is about. It is conducted for the benefit of the very few, at the expense of the very many."
" A racket is best described, I believe, as something that is not what it seems to the majority of the people. Only a small "inside" group knows what it is about. It is conducted for the benefit of the very few, at the expense of the very many."
OP
OP
Midpack
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
It doesn’t but keep pounding that drum.This supports what I posted before:
NYU scientists: Largest U.S. study of COVID-19 finds obesity the single biggest factor in New York City's hospitalizations
Doctors at NYU Langone Health center conducted the largest study so far of U.S. hospital admissions for COVID-19, focused on New York City. They found obesity, along with age, was the biggest deciding factor in hospital admissions, which may suggest the role of hyper-inflammatory reactions that can happen in those with the disease.
https://www.zdnet.com/article/nyu-s...le-biggest-factor-in-new-york-critical-cases/
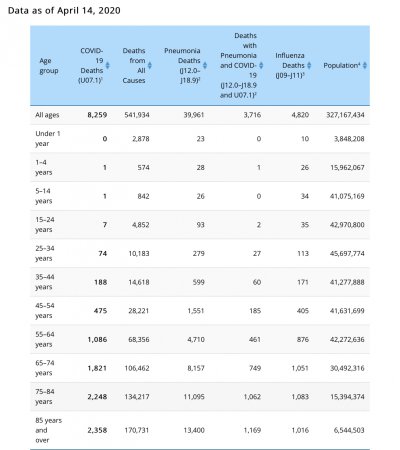
Your link notes obesity is a factor in admissions, it doesn’t say it’s a factor in Covid-19 deaths. The French doctor you quoted was talking about deaths, specifically obese younger people, in America. The table in the OP shows deaths are relatively rare for younger people, period. So far the data does not bear out what your source predicted. Here’s the most recent table below. Obesity undoubtedly contributes to deaths for all ages, but few young people are dying regardless.
78% of deaths are 65 or older, 91% of deaths are 55 and older. The likelihood of death by age group per capita is even more skewed to older cohorts dying. Repeating: With the somewhat loose precautions we've taken, your chances of dying from Covid-19 in the US at age 45-54 yo is 7 in a million (population). At age 35-44 yo is 3 in a million. At age 25-34 it's 1 in a million. At 15-24 it's 1 in 10 million...
Again, underlying health issues is the biggest risk factor (hypertension, heart disease, cancer, diabetes, comprised immune system, obesity, etc.). Age alone isn’t necessarily, but health issues and lower immunity come with age, so it appears age is a risk factor - it appears age is actually secondary.
Attachments
Last edited:
audreyh1
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
I'm not so sure society will heed the message of taking control of one's health. The Type II diabetes epidemic is entirely preventable with a low carb diet and exercise. People continue to ignore that fact.
It would help if the patients were told that by their doctors, but it is still not the mainstream care. In fact it is just barely accepted recently as an alternative, and far from popular among medical practitioners.
Last edited:
Correct, unfortunately. The evidence is clear that minimizing sugar and high carb foods is effective in mitigating metabolic syndrome and Type II diabetes. Doctors are still emphasizing "low fat" as that's still the government focus. How many people have died because of this incorrect paradigm?It would help if the patients were told that by their doctors, but it is still not the mainstream care. In fact it is just barely accepted recently as an alternative, and far from popular.
copyright1997reloaded
Thinks s/he gets paid by the post
^
Anecdotally, reviewing news articles, with photos, of those who have died from this, appears to indicate obesity more often than not.
Yep, the big secret no one wants to discuss (the role of obesity in death rates). I have yet to see any stats regarding BMI and death rates.
ivinsfan
Give me a museum and I'll fill it. (Picasso) Give me a forum ...
- Joined
- Feb 19, 2007
- Messages
- 9,962
I'm not so sure society will heed the message of taking control of one's health. The Type II diabetes epidemic is entirely preventable with a low carb diet and exercise. People continue to ignore that fact.
Not sure what you mean here, yes there would be less cases but not every person that has type 2 , can "fix" it with diet and exercise. If you it wouldn't be as prevalent I agree with you on that one..
- Status
- Not open for further replies.
Similar threads
- Replies
- 44
- Views
- 5K
- Replies
- 7
- Views
- 989
- Replies
- 33
- Views
- 3K