BoodaGazelle
Recycles dryer sheets
- Joined
- Mar 1, 2017
- Messages
- 284
I recently switched doctors. As part of my overall physical, my cholesterol came back high, which I already knew (it runs very high in my family). I had previously been on Crestor (statin) but after losing 30 lbs., decided (with last doctor's blessing) to stop it.
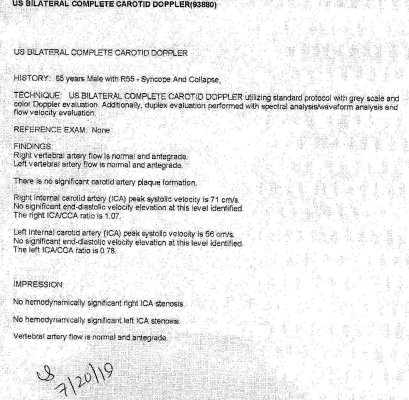
I fully intended to stay off of it, but the new doctor suggested I get a carotid artery scan to look for plaque, and it came back normal on the right bulb, but said this for the left:
Here is my only question. As far as I can tell from searching, the phrase "not hemodynamically significant" means "does not affect blood flow".
But if we were talking about a pipe of some sort that performed a critical function, and it was almost 1/3 to 1/2 blocked, would you think that was not "significant"?
Has anyone else had this type of ultrasound? Can you explain what this means?
I fully intended to stay off of it, but the new doctor suggested I get a carotid artery scan to look for plaque, and it came back normal on the right bulb, but said this for the left:
There is mild-to-moderate plaque in the left carotid bulb. This is associated with 30-49 percent stenosis. This is not hemodynamically significant.
Because of this alone, I agreed to go back on Crestor, which I hate due to muscle tiredness side effects.
Here is my only question. As far as I can tell from searching, the phrase "not hemodynamically significant" means "does not affect blood flow".
But if we were talking about a pipe of some sort that performed a critical function, and it was almost 1/3 to 1/2 blocked, would you think that was not "significant"?
Has anyone else had this type of ultrasound? Can you explain what this means?